
Section 4: Clinical Pearls
4.1 Common Orders
Admission Orders
Electronic ordering often means you won’t be putting in orders directly, but for a few consults you should try writing out practice orders with your consult to compare against your resident’s.
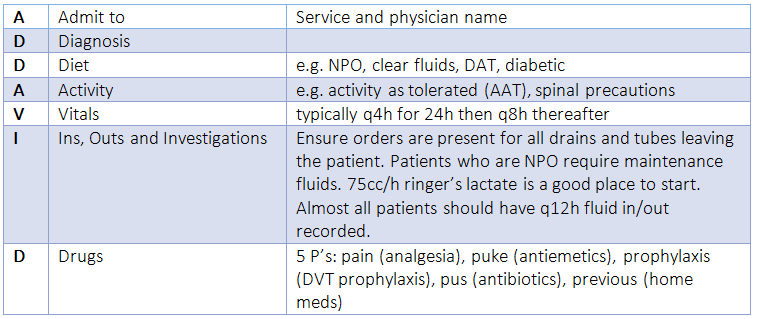
The ADDAVID mnemonic is useful:
Admission Orders
Electronic ordering often means you won’t be putting in orders directly, but for a few consults you should try writing out practice orders with your consult to compare against your resident’s.
The ADDAVID mnemonic is useful:
Discharge Orders and Summary
- Disposition: Where is the patient going? Home, rehab, etc.
- Medications at discharge: Check with your team to make sure antibiotics, analgesics, and any other special meds are prescribed. You do not need to re-prescribe stable home medications.
- Home care: Does the patient need CCAC? Patients with packing, new stomas, requiring physiotherapy, etc.
- See family physician in 1 week to review course in hospital ± staple removal
- See surgeon in N weeks for follow-up
4.2 Common Surgical Post-Op Issues
Review all post-op issues with a resident. Always start with the vitals.
Fever
The differential for fever includes infection, inflammation, and malignancy. In our patients, infection must be ruled out. DVTs and drug/transfusion reactions are possible but less common sources of fever. ‘Surgical inflammation’ or tumor-related malignancy are diagnoses of exclusion. Atelectasis is not a cause of fever.
Start by getting a recent set of vitals and taking a focused history/physical primarily looking for a source of infection (skin/wound, chest, urinary tract, GI tract/abdomen). Be sure to specifically review the WBC trends, last cultures sent and their results, and antibiotic history.
Wound infection
For cellulitis, treat with antibiotics. If there is an abscess, incise and drain. Wash out with sterile saline solution, then pack.
Although rare, necrotizing soft tissue infections can occur as early as postoperative day 0 and are life-threatening. Watch out for grey, ‘dishwater’ discharge coming from wounds, pain out of proportion, and hemodynamic instability.
Low urine output
< 0.5cc/kg/h. Consider prerenal, renal, and postrenal causes. Ensure Foley is functioning if present. Maintain high index of suspicion for prerenal cause (hypovolemia due to sepsis or bleeding) in the surgical patient. Complete a focused assessment looking for associated signs of shock (vitals, abdominal exam, GCS/LOC). Consider bloodwork, fluids, and/or blood transfusion in discussion with team.
Electrolyte Abnormalities
See one of the quick reference apps for doses and parameters for reassessment.
Shortness of breath or chest pain
Examine patient, portable CXR, ECG.
Review all post-op issues with a resident. Always start with the vitals.
Fever
The differential for fever includes infection, inflammation, and malignancy. In our patients, infection must be ruled out. DVTs and drug/transfusion reactions are possible but less common sources of fever. ‘Surgical inflammation’ or tumor-related malignancy are diagnoses of exclusion. Atelectasis is not a cause of fever.
Start by getting a recent set of vitals and taking a focused history/physical primarily looking for a source of infection (skin/wound, chest, urinary tract, GI tract/abdomen). Be sure to specifically review the WBC trends, last cultures sent and their results, and antibiotic history.
Wound infection
For cellulitis, treat with antibiotics. If there is an abscess, incise and drain. Wash out with sterile saline solution, then pack.
Although rare, necrotizing soft tissue infections can occur as early as postoperative day 0 and are life-threatening. Watch out for grey, ‘dishwater’ discharge coming from wounds, pain out of proportion, and hemodynamic instability.
Low urine output
< 0.5cc/kg/h. Consider prerenal, renal, and postrenal causes. Ensure Foley is functioning if present. Maintain high index of suspicion for prerenal cause (hypovolemia due to sepsis or bleeding) in the surgical patient. Complete a focused assessment looking for associated signs of shock (vitals, abdominal exam, GCS/LOC). Consider bloodwork, fluids, and/or blood transfusion in discussion with team.
Electrolyte Abnormalities
See one of the quick reference apps for doses and parameters for reassessment.
Shortness of breath or chest pain
Examine patient, portable CXR, ECG.
Upper GI Bleed
Definition: bleeding proximal to the ligament of Treitz (junction between duodenum and jejunum)
Causes:
History:
Key Investigations: CBC, INR/PTT, lytes incl. calcium, group & screen, gastroscopy/CT angiography, more rarely tagged RBC
Initial Management: ABCs, 2 large-bore IVs, NPO, NG tube insertion, IV proton-pump inhibitors, consent and order transfusion if required, CBC q4hr, plan for urgent gastroscopy
Definition: bleeding proximal to the ligament of Treitz (junction between duodenum and jejunum)
Causes:
- Esophagus – varices, Mallory-Weiss tear, esophagitis, cancer
- Stomach – ulcer, gastritis, Dieulafoy’s lesion, cancer
- Duodenum – ulcer, cancer
History:
- Characterize bleed (hematemesis vs coffee grounds; Hx of melena; # episodes and volume)
- Previous GI bleed
- Hx liver disease/EtOH consumption
- Hx protracted vomiting, GERD/epigastric pain
- NSAID and anticoagulant use
- previous surgeries or instrumentation (e.g. gastroscopy)
Key Investigations: CBC, INR/PTT, lytes incl. calcium, group & screen, gastroscopy/CT angiography, more rarely tagged RBC
Initial Management: ABCs, 2 large-bore IVs, NPO, NG tube insertion, IV proton-pump inhibitors, consent and order transfusion if required, CBC q4hr, plan for urgent gastroscopy
Lower GI bleed
Definition: bleeding distal to the ligament of Treitz
Causes:
History:
Key Investigations: CBC, INR/PTT, lytes incl. calcium, group & screen, colonoscopy vs CT angiography site dependent
Initial Management: ABCs, 2 large bore IV, NPO, (call for blood/ consent for transfusion if clinically indicated), CBC q4hr, plan for colonoscopy
Definition: bleeding distal to the ligament of Treitz
Causes:
- Small bowel – angiodysplasia, aortoenteric fistula (ask about history of abdominal aortic aneurysm repair)
- Colon – diverticulosis, colitis (infectious, ischemic, inflammatory), angiodysplasia/arteriovenous malformations, cancer
- Anorectal – hemorrhoids, anal fissure, rectal varices from cirrhosis, cancer
History:
- Characterize bleed (blood on tissue vs blood in toilet; maroon stools vs blood on outside of stool; blood with bowel movement vs spontaneous bleeding; # episodes and volume)
- Pain vs. no pain
- Previous abdominal surgeries
- Personal or family Hx of colon cancer and/or IBD
- Findings on most recent colonoscopy
Key Investigations: CBC, INR/PTT, lytes incl. calcium, group & screen, colonoscopy vs CT angiography site dependent
Initial Management: ABCs, 2 large bore IV, NPO, (call for blood/ consent for transfusion if clinically indicated), CBC q4hr, plan for colonoscopy
Acute Cholecystitis
Definition: inflammation of gallbladder from bile stasis typically due to impacted gallstone, but acalculous in 5-10%. Biliary colic, in contrast, is not associated with inflammation/prolonged impaction of a gallstone.
Presentation: RUQ or epigastric pain, anorexia, nausea/vomiting, fever. Acalculous typically in critically ill patients and is thought to be from shock-induced ischemia to the gallbladder
History: Prior Hx of biliary colic (pattern of post-prandial onset, lasting < 6 hours, +/- nausea/vomiting)
Physical: Murphy’s sign, palpable gallbladder in up to 1/3 of patients
Key Investigations: CBC, LFTs, fractionated bilirubin, ultrasound (98% sensitive)
Definition: inflammation of gallbladder from bile stasis typically due to impacted gallstone, but acalculous in 5-10%. Biliary colic, in contrast, is not associated with inflammation/prolonged impaction of a gallstone.
Presentation: RUQ or epigastric pain, anorexia, nausea/vomiting, fever. Acalculous typically in critically ill patients and is thought to be from shock-induced ischemia to the gallbladder
History: Prior Hx of biliary colic (pattern of post-prandial onset, lasting < 6 hours, +/- nausea/vomiting)
Physical: Murphy’s sign, palpable gallbladder in up to 1/3 of patients
Key Investigations: CBC, LFTs, fractionated bilirubin, ultrasound (98% sensitive)
- Findings of acute cholecystitis on U/S:
- Calculi in the gallbladder
- Anterior gallbladder wall thickening > 3-4 mm
- Pericholecystic fluid
- Gallbladder distension
- Hypervascularization of the gallbladder wall on Doppler
- Positive sonographic Murphy’s sign
Ascending Cholangitis
Definition: obstruction of common bile duct (CBD) (choledocholithiasis 60%, stricture, mass) leading to biliary stasis, bacterial overgrowth and biliary sepsis; KEEPS bacteria most common
Presentation:
Key Investigations: CBC, blood cultures, LFTs, fractionated bilirubin (expect high conjugated bilirubin), lipase (more specific than amylase), ultrasound (best first test), CT/MRCP
Initial Management: Early IV fluid resuscitation and broad-spectrum antibiotics, NPO, +/- NG tube; some patients may require ICU admission. Admit and plan for ERCP + sphincterotomy (treatment of choice); percutaneous trans-hepatic cholangiogram (PTC) and drain if ERCP unavailable. Plan for cholecystectomy if caused by stones.
Definition: obstruction of common bile duct (CBD) (choledocholithiasis 60%, stricture, mass) leading to biliary stasis, bacterial overgrowth and biliary sepsis; KEEPS bacteria most common
Presentation:
- Charcot’s Triad: fever, RUQ pain, jaundice (full triad present in 70% of cases)
- Reynaud’s pentad: fever, RUQ pain, jaundice, hypotension, confusion
- (may have associated nausea and vomiting)
- Acholic stools, tea coloured urine
- Hx of gallstones, biliary colic
- Hx of ulcerative colitis/primary sclerosing cholangitis (PSC)
- Systemic symptoms (fever, chills, sweats)
Key Investigations: CBC, blood cultures, LFTs, fractionated bilirubin (expect high conjugated bilirubin), lipase (more specific than amylase), ultrasound (best first test), CT/MRCP
Initial Management: Early IV fluid resuscitation and broad-spectrum antibiotics, NPO, +/- NG tube; some patients may require ICU admission. Admit and plan for ERCP + sphincterotomy (treatment of choice); percutaneous trans-hepatic cholangiogram (PTC) and drain if ERCP unavailable. Plan for cholecystectomy if caused by stones.
Acute Pancreatitis
Definition: inflammation of pancreas
Presentation: epigastric pain radiating to back, nausea/vomiting, jaundice, fever
History
Key Investigations: CBC, lipase, fractionated bilirubin, AST/ALT/ALP (increased WBC, amylase/lipase, increased liver enzymes points to gallstone pancreatitis), ultrasound, CT for complications
Initial Management: IV fluids, NPO, +/- NG tube, +/- Foley catheter, analgesia, start on CIWA protocol if EtOH withdrawal. May require ICU admission. Antibiotics if evidence of an infection (gas in pseudocyst or pancreatic bed) or concurrent cholangitis.
No role for NPO specifically for pancreatitis. Plan for ERCP if gallstone does not pass on its own.
Definition: inflammation of pancreas
- Atlanta Classification:
- Mild: absence of organ failure or systemic complications (most common)
- Moderately severe: transient organ failure (resolving in < 48 hours), +/- local or systemic complications
- Severe: persistent multi organ failure
Presentation: epigastric pain radiating to back, nausea/vomiting, jaundice, fever
History
- Pain relieved with sitting forward (Ingelfinger’s sign)
- History of gallstones, biliary colic
- EtOH use, medications
- Recent surgery/ instrumentation i.e. ERCP
- Recent trauma
Key Investigations: CBC, lipase, fractionated bilirubin, AST/ALT/ALP (increased WBC, amylase/lipase, increased liver enzymes points to gallstone pancreatitis), ultrasound, CT for complications
Initial Management: IV fluids, NPO, +/- NG tube, +/- Foley catheter, analgesia, start on CIWA protocol if EtOH withdrawal. May require ICU admission. Antibiotics if evidence of an infection (gas in pseudocyst or pancreatic bed) or concurrent cholangitis.
No role for NPO specifically for pancreatitis. Plan for ERCP if gallstone does not pass on its own.
Appendicitis
Definition: appendiceal infection thought to be caused by luminal obstruction
Causes: lymphatic hyperplasia in kids; fecaliths, neoplasms, or unknown in adults
Presentation: nausea/vomiting, anorexia, migratory pain to RLQ, fever
History: Progression of symptoms (typically abdominal pain, then anorexia, then nausea/vomiting) – Alvarado score notes all the high likelihood ratio clinical features of appendicitis though we don’t generally use the score to make decisions
Physical: tenderness at McBurney’s point, Rovsing’s sign, psoas sign, obturator sign
Investigations: CBC, urinalysis, beta hCG, ultrasound, CT if concern for complicated appendicitis or when ultrasound not feasible/inconclusive, consider MRI in pregnancy
Definition: appendiceal infection thought to be caused by luminal obstruction
Causes: lymphatic hyperplasia in kids; fecaliths, neoplasms, or unknown in adults
Presentation: nausea/vomiting, anorexia, migratory pain to RLQ, fever
History: Progression of symptoms (typically abdominal pain, then anorexia, then nausea/vomiting) – Alvarado score notes all the high likelihood ratio clinical features of appendicitis though we don’t generally use the score to make decisions
Physical: tenderness at McBurney’s point, Rovsing’s sign, psoas sign, obturator sign
Investigations: CBC, urinalysis, beta hCG, ultrasound, CT if concern for complicated appendicitis or when ultrasound not feasible/inconclusive, consider MRI in pregnancy
- Findings on U/S:
- dilation >6-7mm
- hyperemia, echogenic periappendiceal fat, periappendiceal fluid
- non-compressible appendix
- fecalith
Mechanical Small Bowel Obstruction
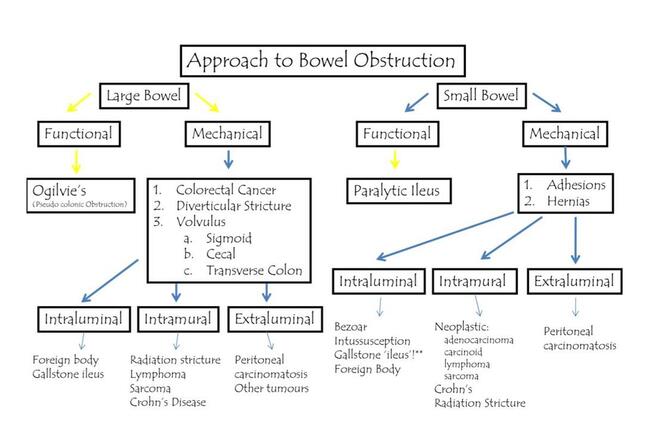
Dr. Darlene Fenech, Large and Small Bowel Obstruction, 2017
Definition: obstruction resulting in the build-up of fluid and gas proximally with decompression of bowel distally; increases in intraluminal and intramural pressure may result in impaired perfusion leading to intestinal ischemia
Classification:
History:
Goal of eliciting underling cause: any previous abdominal surgeries, hernias, family or personal history of colorectal cancer, history of IBD
Complete vs incomplete obstruction: last BM, last flatus
Physical: Vitals (abnormal vital signs increase suspicion of strangulation/ ischemia), abdominal distension, tenderness (focal vs diffuse), peritonitis
Investigations: CBC, lytes, lactate
Definition: obstruction resulting in the build-up of fluid and gas proximally with decompression of bowel distally; increases in intraluminal and intramural pressure may result in impaired perfusion leading to intestinal ischemia
Classification:
- Partial SBO: lumen partially occluded allowing some passage of fluid and gas
- Complete SBO: lumen fully occluded preventing passage of any fluid or gas
- Closed-loop obstruction: segment of small intestine is obstructed proximally and distally creating a loop of bowl from which fluid and gas cannot escape resulting in high risk of perforation
- Adhesions (most common), hernias, cancers, strictures, volvulus
History:
Goal of eliciting underling cause: any previous abdominal surgeries, hernias, family or personal history of colorectal cancer, history of IBD
Complete vs incomplete obstruction: last BM, last flatus
Physical: Vitals (abnormal vital signs increase suspicion of strangulation/ ischemia), abdominal distension, tenderness (focal vs diffuse), peritonitis
Investigations: CBC, lytes, lactate
- Imaging:
- AXR: distension of small bowel > 3cm, decompressed distal loops, paucity of air in the colon, air fluid levels
- CXR: best (most rapid) initial imaging to r/o pneumoperitoneum
- CT: further characterizes SBO, identifies transition zone, and evaluates for signs of ischemia
- Findings consistent with ischemia = decreased bowel wall enhancement, mural thickening, pneumatosis, mesenteric edema/ congestion/hemorrhage, free fluid, portal venous gas
Diverticulitis
Definition: inflammation of a diverticula leading to focal necrosis which may result in local perforation; 95% left sided in Western nations
Cause: erosion of wall secondary to increased intraluminal pressure or inspissated food particles
Presentation: LLQ pain, changes in bowel habits, nausea/vomiting, fever
History: age, previous colonoscopy
Physical: presence of peritonitis key to management, focal vs diffuse
Investigations: CBC, upright CXR for free air, CT (signs include presence of diverticuli, fat stranding, colonic wall thickening, abscess, fistula, extraluminal air)
Initial Management: usually non-operative in the absence of generalized peritonitis, free perforation on imaging, or failure of medical management. Patients with abscesses need follow-up colonoscopy to rule out malignancy.
Definition: inflammation of a diverticula leading to focal necrosis which may result in local perforation; 95% left sided in Western nations
Cause: erosion of wall secondary to increased intraluminal pressure or inspissated food particles
Presentation: LLQ pain, changes in bowel habits, nausea/vomiting, fever
History: age, previous colonoscopy
Physical: presence of peritonitis key to management, focal vs diffuse
Investigations: CBC, upright CXR for free air, CT (signs include presence of diverticuli, fat stranding, colonic wall thickening, abscess, fistula, extraluminal air)
Initial Management: usually non-operative in the absence of generalized peritonitis, free perforation on imaging, or failure of medical management. Patients with abscesses need follow-up colonoscopy to rule out malignancy.
Mesenteric Ischemia
Definition: acute ischemia of bowel secondary to reduced blood flow through mesenteric vasculature
Causes:
History: Elicit history of predisposing conditions i.e. atrial fibrillation, peripheral vascular disease
Physical: pain out of proportion to exam, peritoneal signs late in course
Investigations: CBC, lactate, CTA
Definition: acute ischemia of bowel secondary to reduced blood flow through mesenteric vasculature
Causes:
- Arterio-occlusive mesenteric ischemia: thrombus, embolus, extrinsic compression
- Non-occlusive mesenteric ischemia: vasoconstriction secondary to hypoperfusion
- Mesenteric venous thrombosis
History: Elicit history of predisposing conditions i.e. atrial fibrillation, peripheral vascular disease
Physical: pain out of proportion to exam, peritoneal signs late in course
Investigations: CBC, lactate, CTA
- CT findings consistent with ischemia = decreased bowel wall enhancement, mural thickening, pneumatosis, mesenteric edema/ congestion/hemorrhage, free fluid, portal venous gas
Perforated Viscus
Definition: perforation within the gastrointestinal tract resulting in peritonitis and gross spillage of intestinal contents
Causes:
History: Goal of identifying the underlying cause (surgical history, NSAID use, Hx of ulcers, history in keeping with SBO/appendicitis/diverticulitis, travel history, Hx of IBD, recent instrumentation)
Physical: vitals and peritonitis
Investigations: CBC, lytes, lactate, blood cultures, upright CXR, CT uncommonly ordered by general surgery given management is surgical regardless and patients are typically unstable
Initial Management: IV fluids, NG tube, broad spectrum antibiotics, NPO, volume resuscitation and correction of electrolyte derangements prior to surgery; operative management
Definition: perforation within the gastrointestinal tract resulting in peritonitis and gross spillage of intestinal contents
Causes:
- Esophagus: Boerhaave's syndrome, foreign body
- Stomach, duodenum: peptic ulcers
- Small bowel: closed loop bowel obstruction, mesenteric ischemia
- Colon: Appendicitis, diverticulitis, colitis, iatrogenic (e.g. colonoscopy)
History: Goal of identifying the underlying cause (surgical history, NSAID use, Hx of ulcers, history in keeping with SBO/appendicitis/diverticulitis, travel history, Hx of IBD, recent instrumentation)
Physical: vitals and peritonitis
Investigations: CBC, lytes, lactate, blood cultures, upright CXR, CT uncommonly ordered by general surgery given management is surgical regardless and patients are typically unstable
Initial Management: IV fluids, NG tube, broad spectrum antibiotics, NPO, volume resuscitation and correction of electrolyte derangements prior to surgery; operative management
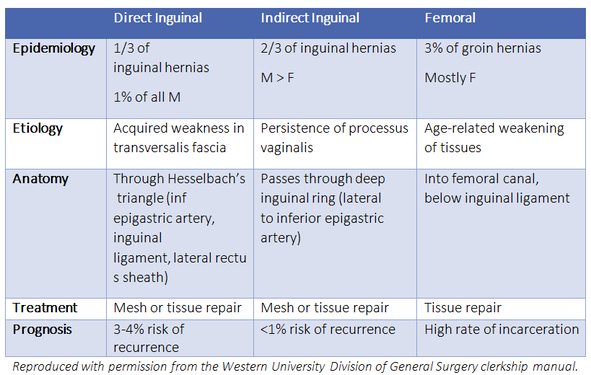
Groin Hernias
Contents of the spermatic cord: vas deferens, testicular artery, pampiniform plexus, cremaster muscle, lymphatics, genital branch of genitofemoral nerve
Contents of the spermatic cord: vas deferens, testicular artery, pampiniform plexus, cremaster muscle, lymphatics, genital branch of genitofemoral nerve
Breast Cancer
Epidemiology: 1/8 women will be diagnosed, 2nd leading cause of cancer mortality in women
Risk factors: Female sex, older age, personal/family breast cancer history, early menarche, late menopause, HRT/OCP, BRCA1/2, alcohol, obesity
Investigations:
Epidemiology: 1/8 women will be diagnosed, 2nd leading cause of cancer mortality in women
Risk factors: Female sex, older age, personal/family breast cancer history, early menarche, late menopause, HRT/OCP, BRCA1/2, alcohol, obesity
Investigations:
- Imaging: mammography, ultrasound. MRI and staging studies (CT, bone scan) in advanced disease only
- Pathology: Core biopsy
Benign Breast Disease
Common Features: breast pain, focal areas of nodularity or cysts often in the upper outer quadrant, frequently bilateral, mobile, varies with menstrual cycle, non-bloody nipple discharge
DDx Benign breast mass: fibrocystic changes, fibroadenoma, abscess, lipoma, papilloma, many others
Management: reassurance, surveillance, imaging (mammogram/ultrasound), biopsy
Common Features: breast pain, focal areas of nodularity or cysts often in the upper outer quadrant, frequently bilateral, mobile, varies with menstrual cycle, non-bloody nipple discharge
DDx Benign breast mass: fibrocystic changes, fibroadenoma, abscess, lipoma, papilloma, many others
Management: reassurance, surveillance, imaging (mammogram/ultrasound), biopsy
Bariatric Surgery
- Part of a multidisciplinary team treating morbid obesity.
- Criteria in Ontario include:
- BMI >40 or BMI >35 with obesity-related health problem (e.g. HTN, OSA, T2DM)
- Previous weight loss attempts
- Psychologically and medically fit (multidisciplinary approach)
- Non-smoker, no substance misuse
- Main weight reduction surgery options: Roux-en-Y gastric bypass (RYGB), sleeve gastrectomy
- The mechanism by which gastric bypass causes weight loss includes restrictive and malabsorptive components
- Late Complications of RYGB: marginal ulcer, internal hernia, vitamin/mineral deficiencies
Pancreatic cancer
Epidemiology: M:F 1.3:1; average age 50-70
Classic presentation: painless jaundice, palpable gallbladder, weight loss
Risk factors: Smoking (most established modifiable risk factor), alcohol, Age, DM, chronic pancreatitis
Types: pancreatic adenocarcinoma (most common), intraductal papillary mucinous neoplasm (IPMN), others. NOTE: cholangiocarcinoma (bile duct cancer) is often indistinguishable on imaging.
Treatment options:
Epidemiology: M:F 1.3:1; average age 50-70
Classic presentation: painless jaundice, palpable gallbladder, weight loss
Risk factors: Smoking (most established modifiable risk factor), alcohol, Age, DM, chronic pancreatitis
Types: pancreatic adenocarcinoma (most common), intraductal papillary mucinous neoplasm (IPMN), others. NOTE: cholangiocarcinoma (bile duct cancer) is often indistinguishable on imaging.
Treatment options:
- Whipple procedure (pancreaticoduodenectomy): removal of duodenum, proximal pancreas, gallbladder, common bile duct, and distal stomach. Bile duct, pancreas, and stomach are each respectively anastomosed with jejunum.
- Adjuvant chemotherapy is standard of care
- Neoadjuvant chemotherapy if tumor is close to vital structures.
- Chemotherapy/radiation if tumor is unresectable (e.g. distant mets, involvement of SMA/SMV)
Benign Perianal Disease
3 main causes of acute anal pain: Thrombosed external hemorrhoid, anal fissure, and perianal abscess
3 main causes of acute anal pain: Thrombosed external hemorrhoid, anal fissure, and perianal abscess
- Anal fissure: painful tear below dentate line, blood streaks on stool, classically has fear to pass gas due to pain
- Pathophysiology: High resting anal tone that causes local ischemia and prevents healing of acute tear, usually caused by constipation
- Management: soften stool, topical calcium channel blockers, less commonly botulinum toxin or sphincterotomy.
- Anorectal abscess: arise from blocked anal glands, classified by anatomical relationship to the sphincter muscles
- Management: incision and drainage, healing by secondary intention.
- Fistula-in-ano: abnormal communication between epithelialized surfaces of rectum and perianal skin, usually originating from an abscess that has been drained
- Management: examination under anesthesia with seton placement or fistulotomy.
- Rectal prolapse: protrusion of rectal mucosa through external sphincter
- Management: conservative (stool softening, manual reduction) and surgery (various approaches)
Hemorrhoids
Pathogenesis: Three venous cushions that line the anal canal — the left lateral, right anterior, and right posterior positions.
Classification:
Management: diet high in soluble fiber (Metamucil) and water, steroid cream, Sitz bath, band ligation, hemorroidectomy
Pathogenesis: Three venous cushions that line the anal canal — the left lateral, right anterior, and right posterior positions.
Classification:
- Internal hemorrhoids
- Location: above dentate line
- Presentation: painless bleeding, prolapse
- Subclassification:
- Class I = no prolapse
- Class II = prolapse with spontaneous reduction
- Class III = prolapse requiring manual reduction
- Class IV = permanent prolapse
- External hemorrhoids:
- Location: located below dentate line
- Presentation: itching, pain, bleeding, prolapse, thrombosis
Management: diet high in soluble fiber (Metamucil) and water, steroid cream, Sitz bath, band ligation, hemorroidectomy
Colorectal Cancer
Epidemiology: 4th most common cancer, 2nd highest cancer mortality, 7% lifetime risk in Canadian population
Risk factors: age, genetic (FAP, HNPCC), ulcerative colitis, diet, smoking
Features: often asymptomatic, occult bleeding, abdominal pain, weight loss, bowel changes, symptoms of distant metastases
Investigations: colonoscopy (gold standard), FOBT/FIT occult blood tests, CT colonography, staging CT C/A/P
Treatment:
Epidemiology: 4th most common cancer, 2nd highest cancer mortality, 7% lifetime risk in Canadian population
Risk factors: age, genetic (FAP, HNPCC), ulcerative colitis, diet, smoking
Features: often asymptomatic, occult bleeding, abdominal pain, weight loss, bowel changes, symptoms of distant metastases
Investigations: colonoscopy (gold standard), FOBT/FIT occult blood tests, CT colonography, staging CT C/A/P
Treatment:
- Colon: curative resection with wide margins based on blood supply and lymphatics (e.g. right/left hemicolectomy), adjuvant chemotherapy in stage III and some stage II, palliative chemotherapy/radiation/surgery for hemorrhage/obstruction.
- Rectum: curative resection, options include local excision (rare), low anterior resection (LAR) if adequate distal margin to spare sphincter, abdominoperineal resection (APR) if inadequate distal margin. Neoadjuvant chemoradiotherapy for locally advanced rectal cancers (not colon).
4.6 Trauma Surgery
Primary survey
The initial resuscitation follows principles laid out by ATLS and the ABCDE format.
While the approach to the primary and secondary survey is usually taught in a stepwise fashion, at SMH and SHSC the trauma team is typically large enough that all components of the primary and secondary survey may appear to be done in parallel!
For your own learning, try to run through a stepwise assessment in your head for each patient that comes in through the trauma bay.
Primary survey
The initial resuscitation follows principles laid out by ATLS and the ABCDE format.
- Airway
- Always assessed maintaining C-spine precautions
- 2 main indications for intubation
- Anatomic
- Obstruction (blood, vomit, hematoma)
- Disruption of airway (laryngeal fracture, facial fracture, transection)
- Neurologic
- Low GCS (<8)
- High C-spine injury
- Anatomic
- Intubation is performed using in-line stabilization for C-spine
- Breathing
- Auscultation, palpation, and CXR to assess for 5 life-threatening injuries
- Tension pneumothorax
- Open pneumothorax
- Flail chest/pulmonary contusion
- Massive hemothorax
- Cardiac tamponade
- Tension/open pneumothorax and hemothorax require chest tube
- Tamponade requires paracentesis or pericardial window
- Severe flail chest may require intubation and positive pressure ventilation to relieve work of breathing and pain
- Auscultation, palpation, and CXR to assess for 5 life-threatening injuries
- Circulation
- Focused assessment to rule out 5 locations of life-threatening bleeding
- External – examine entire body
- Chest – physical exam and CXR
- Abdomen – physical exam and FAST
- Pelvis – pelvic stability and pelvic X-ray
- Long bones – physical exam
- Direct pressure +/- tourniquet for external bleeding
- Splint long bone fractures
- Pelvic binder for pelvic fractures
- Focused assessment to rule out 5 locations of life-threatening bleeding
- Disability
- Focused neurologic exam for head and spinal cord injury
- GCS
- Pupils
- Lateralizing signs
- Traumatic brain injury divided into severe (GCS<8), moderate (9-12), and mild (13-15)
- Cushing’s response to increased ICP – bradycardia, hypertension, irregular breathing
- Focused neurologic exam for head and spinal cord injury
- Exposure
- Must examine every part of patient’s body
- Remove all articles of clothing
- Logroll patient to look at back and perineum
While the approach to the primary and secondary survey is usually taught in a stepwise fashion, at SMH and SHSC the trauma team is typically large enough that all components of the primary and secondary survey may appear to be done in parallel!
For your own learning, try to run through a stepwise assessment in your head for each patient that comes in through the trauma bay.
4.7 Operative Pearl
Introduction
We’ve listed several common operations with their indications and answers to frequently asked questions about the procedure.
This is not a comprehensive list of procedures or an exhaustive list of their indications. Surgical Recall is a frequently recommended, more comprehensive source of answers to ‘greatest hits’ intraoperative questions, such as ‘If a normal appendix is found upon exploration, should you take out the normal appendix?’ (Yes!). However, some of it is not consistent with what you’ll see in Toronto, so we’ve done our best to build on Surgical Recall using local practices/best evidence where possible.
Introduction
We’ve listed several common operations with their indications and answers to frequently asked questions about the procedure.
This is not a comprehensive list of procedures or an exhaustive list of their indications. Surgical Recall is a frequently recommended, more comprehensive source of answers to ‘greatest hits’ intraoperative questions, such as ‘If a normal appendix is found upon exploration, should you take out the normal appendix?’ (Yes!). However, some of it is not consistent with what you’ll see in Toronto, so we’ve done our best to build on Surgical Recall using local practices/best evidence where possible.
Appendectomy
Indication: appendicitis, interval appendectomy after perforated appendicitis, appendiceal neoplasm
Pearls:
Indication: appendicitis, interval appendectomy after perforated appendicitis, appendiceal neoplasm
Pearls:
- Almost always laparoscopic. May see open appendectomy for physiologic (e.g. patient in extremis) or anatomic (e.g. horrible inflammation makes laparoscopic dissection unsafe) reasons.
- Antibiotics are stopped postoperatively if the appendix was not perforated. A fixed course of 4 days of antibiotics (often Amoxicillin-Clavulinate 875/125 PO BID) is otherwise generally appropriate.
- Structures to be wary of: cecum, terminal ileum, ileocecal valve, ureter, iliac artery
Cholecystectomy
Indication: symptomatic cholelithiasis (cholecystitis, gallstone pancreatitis, etc.), gallbladder cancer/polyp
Pearls:
Indication: symptomatic cholelithiasis (cholecystitis, gallstone pancreatitis, etc.), gallbladder cancer/polyp
Pearls:
- The critical view of safety must be achieved before clipping to reduce bile duct injury rates (great instructional video for standard lap chole - here)
- Structures to worry about: common bile duct, right hepatic artery, duodenum
Inguinal hernia repair
Indication: symptomatic inguinal hernia
Pearls:
Indication: symptomatic inguinal hernia
Pearls:
- Many variations – Lichtenstein (tension-free mesh repair) one of the most common. Tissue repairs (Bassini, McVay) harder to do and less common, other than in emergency situations where contamination of mesh by ischemic bowel is a concern
- Structures to worry about: femoral vessels, vas deferens in men, ilioinguinal nerve
Lumpectomy
Indication: Benign and malignant etiologies, used in conjunction with radiation and sentinel node biopsy for breast cancer
Pearls:
Indication: Benign and malignant etiologies, used in conjunction with radiation and sentinel node biopsy for breast cancer
Pearls:
- Non-palpable abnormalities are marked by radiology with a wire or radioactive seed
Simple mastectomy
Indication: Invasive breast cancer, extensive DCIS, contraindications to lumpectomy
Pearls:
Indication: Invasive breast cancer, extensive DCIS, contraindications to lumpectomy
Pearls:
- Borders of the breast dissection: clavicle superiorly, sternum medially, inframammary fold inferiorly, anterior border of latissimus dorsi laterally
- Dissection ends posteriorly at the fascia of the pec muscle
Colectomy
Indication: many – infectious (e.g. diverticulitis), inflammatory (e.g. IBD), structural (e.g. volvulus, malignant (e.g. CRC), vascular (e.g. ischemic bowel), etc.
Pearls:
Indication: many – infectious (e.g. diverticulitis), inflammatory (e.g. IBD), structural (e.g. volvulus, malignant (e.g. CRC), vascular (e.g. ischemic bowel), etc.
Pearls:
- Hemicolectomy can be left or right, subtotal colectomy leaves the rectum, total colectomy takes the rectum
- Know the vascular supply to the colon and the watershed areas
- Structures to worry about: depends on the indication and exactly what part of the colon you’re taking out but the ureters are almost always a concern
Roux-en-Y
Indication: used for upper GI reconstruction, most commonly as a gastric bypass for obesity, but applicable in many other scenarios (e.g. gastric cancer)
Pearls:
Indication: used for upper GI reconstruction, most commonly as a gastric bypass for obesity, but applicable in many other scenarios (e.g. gastric cancer)
Pearls:
- roux limb = feeding limb; Y limb = biliary limb
- lower threshold for operation in patients presenting with obstruction and a history of Roux-en-Y reconstruction than for patients with typical presumed adhesive SBO – complex anatomy can result in internal hernias despite normal CT
4.8 Miscellaneous Advice
- Generally, issues related to patient care should be escalated up the hierarchy in order. If you’re worried about something, try reaching your junior and senior first before directly contacting your staff.
- Most of the time, life on surgery clerkship isn’t as bad as it’s rumored to be – but sometimes it is. For those times when your daily schedule doesn’t obey typical societal conventions, a good rule of thumb is to eat when your residents eat and sleep when your residents sleep. If your residents say they’re going to go nap or grab a bite, there’s nothing wrong with asking to do the same. Occasionally, it may be the case that nobody has time for a full meal – come prepared with an energy bar or 3 so that you can eat on the go.