
5.1 Consult Note
ID
RFR
The reason you were called (i.e. the presumed diagnosis, what they are asking the surgical team to rule out or manage)
HPI
Complete list of medical conditions. Noting severity where applicable is helpful to determine whether someone might require optimization or the involvement with another service (Anesthesia, Internal Medicine) before proceeding with surgery. Often important to know if the patient has had a scope before.
PSHx
Always ask about previous surgeries! Helpful to know indication, approach, and surgeon/hospital.
Medications
Helpful to get the doses if the patient is going to be admitted as the team will have to order these.
Allergies
Social Hx
Smoking, EtOH, recreational drugs, travel, sick contacts
Important to get to know your patient a little bit. It is nice to know what they do and who they live with to give you a sense of how their surgical problem will impact their life.
Family Hx
IBD, cancers
O/E
Crucial to note what if any management has been initiated by the ED in the interval between most recent vitals and vitals at presentation. A patient who’s unstable after 3L of crystalloid and antibiotics is different from a patient who’s unstable without having received any intervention!
List of the investigations that have been done so far
This is typically a collaborative effort between you and your resident
ID
RFR
The reason you were called (i.e. the presumed diagnosis, what they are asking the surgical team to rule out or manage)
HPI
- Brief description of what ultimately prompted the patient to present to the hospital
- Characterize pain (OPQRST)
- Associated symptoms (appetite/nausea/ vomiting, BMs/flatus, hematochezia/hematemesis/ melena, fevers/chills)
- Previous tests done prior to presentation, if any (i.e. most recent colonoscopy results)
- Risk factors
- Relevant and brief review of systems
Complete list of medical conditions. Noting severity where applicable is helpful to determine whether someone might require optimization or the involvement with another service (Anesthesia, Internal Medicine) before proceeding with surgery. Often important to know if the patient has had a scope before.
PSHx
Always ask about previous surgeries! Helpful to know indication, approach, and surgeon/hospital.
Medications
Helpful to get the doses if the patient is going to be admitted as the team will have to order these.
Allergies
Social Hx
Smoking, EtOH, recreational drugs, travel, sick contacts
Important to get to know your patient a little bit. It is nice to know what they do and who they live with to give you a sense of how their surgical problem will impact their life.
Family Hx
IBD, cancers
O/E
Crucial to note what if any management has been initiated by the ED in the interval between most recent vitals and vitals at presentation. A patient who’s unstable after 3L of crystalloid and antibiotics is different from a patient who’s unstable without having received any intervention!
- Vitals (give a Tmax, vitals on presentation to ED and most recent set of vitals)
- General appearance (in distress/discomfort vs NAD)
- Abdominal exam:
- Appearance (i.e. +/- distension, stigmata of liver disease, presence of surgical scars)
- Percussion (i.e. tympanic if distended, tenderness to percussion)
- Palpation (i.e. soft vs rigid; describe the location of maximal tenderness vs. non-tender)
- Presence or absence of special signs (Murphy’s, obturator, psoas, Rovsing’s, etc.)
- Peritoneal signs: shake tenderness, rigidity, tenderness to percussion, rebound tenderness, guarding, referred pain
- Digital Rectal Exam: may be best to wait and do this together with your resident so as not to subject the patient to an uncomfortable exam more than once (comment on +/- blood, hemorrhoids, fissures, palpable masses)
List of the investigations that have been done so far
- Blood work (document abnormal and clinically important results)
- Imaging (document summary of U/S or CT scan findings)
This is typically a collaborative effort between you and your resident
- Summary sentence of who the patient is and what the most pressing issues are
- Presumptive diagnosis and potential underlying etiology
- Plan: where the patient is going (admission vs discharge); further investigations required (imaging, repeat lab work); initial management (i.e. NPO, NG tube insertion, antibiotics, IV fluids, medications etc.); planned interventions (i.e. surgery), follow-up plan (especially if patient is being discharged home)
- Your hand-written consult note in the patient’s chart with your residents co-signature
- +/- dictation (some hospitals will require that you dictate your consult note)
- Sign out list (your resident may ask you to add a patient that you saw and admitted to the team’s list with a very brief description of their presentation and initial management)
- Discharge summary (only if you have free time, it may be helpful to open a discharge summary for the patients you admit to add a brief summary of their presentation to hospital)
5.2 Dictation
General Tips
General Tips
- It may help to type out or write down your first few dictations or dictations about complicated cases – this will also help you ensure you have all the details you need before you sit down at the phone!
- Learn how to pause the dictation to collect your thoughts!
- If you forgot something 2 paragraphs ago, just tell the transcriber to add the parts you’ve forgotten in the section above
- Write down your dictation codes so you can reference or edit them later
- All punctuation and paragraph breaks need to be dictated (e.g. ‘new line’, ‘period’)
- “This is [your name], spelled [spell your name], dictating a [consult/progress] note on behalf of Dr. [attending’s name], spelled [spell attending’s name]
- Patient’s name is [patient name], spelled [spell patient’s name]. MRN is [MRN], date of birth [DOB].
- Please copy to [family physician, other relevant physicians].
- Date of the clinic/consultation is [date].
- “New line It was a pleasure being involved in this patient’s care period New line Sincerely New line [your name] End dictation”
5.3 SOAP note
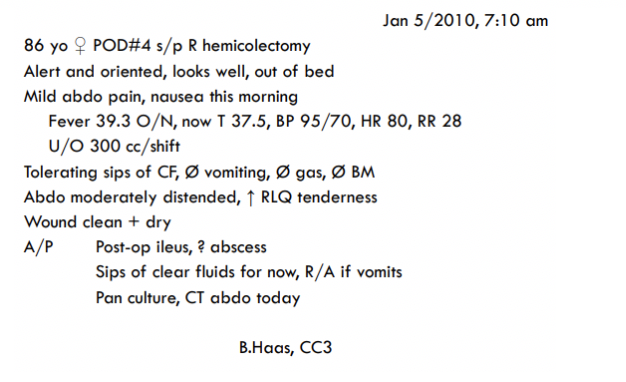
SOAP stands for Subjective, Objective, Assessment, and Plan and outlines the format of your notes on inpatient rounds. Most commonly you’ll be rounding on patients with abdominal pathology, so we’ve outlined an approach to a note with that in mind. In general, we ask the same questions of almost every patient on rounds with an abdominal pathology. For interpretability and brevity, take notes that describe symptoms/signs as present or absent. If present, a trend is useful - better, worse, or the same. Writing in full sentences is not necessary and will slow you down.
The chart is a medicolegally important document that other team members and health professionals will use for patient care. If you’re not sure about what to write for a specific finding or plan, ask a resident to clarify.
Finally, when in doubt, remember the ‘midnight rule’ – what would the on-call team need to know if this patient suddenly got sick in the middle of the night?
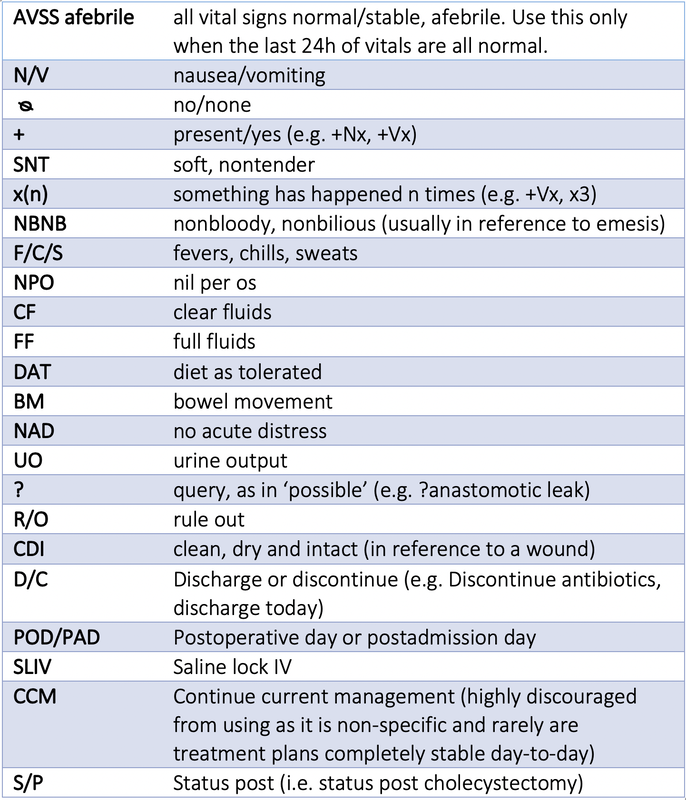
Useful Acronyms and Abbreviations for Notetaking
Note: most of these are universal and you’ll see them on other services, but if a member of the healthcare team takes issue with using any of these abbreviations it’s best to follow their advice as local practices vary.
SOAP stands for Subjective, Objective, Assessment, and Plan and outlines the format of your notes on inpatient rounds. Most commonly you’ll be rounding on patients with abdominal pathology, so we’ve outlined an approach to a note with that in mind. In general, we ask the same questions of almost every patient on rounds with an abdominal pathology. For interpretability and brevity, take notes that describe symptoms/signs as present or absent. If present, a trend is useful - better, worse, or the same. Writing in full sentences is not necessary and will slow you down.
The chart is a medicolegally important document that other team members and health professionals will use for patient care. If you’re not sure about what to write for a specific finding or plan, ask a resident to clarify.
Finally, when in doubt, remember the ‘midnight rule’ – what would the on-call team need to know if this patient suddenly got sick in the middle of the night?
Useful Acronyms and Abbreviations for Notetaking
Note: most of these are universal and you’ll see them on other services, but if a member of the healthcare team takes issue with using any of these abbreviations it’s best to follow their advice as local practices vary.
SOAP Framework: Formatting
All notes should include a header with essential demographic information:
Pain:yes/no, how bad out of 10, getting worse, improving
Nausea/vomiting:yes/no, quantity
Flatus/BMs:yes/no, quantity
Eating:if eating, are they tolerating ice chips/CF/FF/DAT?
Ambulating:sitting at edge of bed, walking down the hall, 3 laps around the hall, etc.
SOAP Framework: Objective
Vital signs:AVSS/AVSN afebrile if well. A good general approach to documenting abnormal vitals is Tmax with most abnormal vitals and most recent vitals.
Ins and outs:stomas, JP drains, Foleys, chest tubes, etc.
End-of-the-bed assessment:toxic/nontoxic, no distress, diaphoretic, sleeping, etc.
Wound exam:swelling, discharge, erythema. Normal = clean, dry, and intact.
Abdominal exam:
Your assessment on rounds generally reaches one of two mutually exclusive conclusions, and this constitutes your assessment:
1) There are no red flags of failure to progress or complications, and the patient is progressing appropriately with their treatment or appropriate for their postoperative day
2) Something is not right and you’re worried about, querying, or trying to rule out some complication or condition
SOAP Framework: Plan
Should logically follow from the assessment.
If we’re worried about complication X (e.g. anastomotic leak), what are we doing to rule it out
All notes should include a header with essential demographic information:
- Your service; in this case, General Surgery
- Date
- Patient age and sex
- Post-op or post-admit day
- Diagnosis
Pain:yes/no, how bad out of 10, getting worse, improving
Nausea/vomiting:yes/no, quantity
Flatus/BMs:yes/no, quantity
Eating:if eating, are they tolerating ice chips/CF/FF/DAT?
Ambulating:sitting at edge of bed, walking down the hall, 3 laps around the hall, etc.
SOAP Framework: Objective
Vital signs:AVSS/AVSN afebrile if well. A good general approach to documenting abnormal vitals is Tmax with most abnormal vitals and most recent vitals.
Ins and outs:stomas, JP drains, Foleys, chest tubes, etc.
End-of-the-bed assessment:toxic/nontoxic, no distress, diaphoretic, sleeping, etc.
Wound exam:swelling, discharge, erythema. Normal = clean, dry, and intact.
Abdominal exam:
- Inspection: distended/nondistended
- Palpation: soft/tense, tender/nontender, peritonitic/nonperitonitic
- Percussion: tympanic, hyperresonant, dull
- Auscultation: not typically done on rounds
Your assessment on rounds generally reaches one of two mutually exclusive conclusions, and this constitutes your assessment:
1) There are no red flags of failure to progress or complications, and the patient is progressing appropriately with their treatment or appropriate for their postoperative day
2) Something is not right and you’re worried about, querying, or trying to rule out some complication or condition
SOAP Framework: Plan
Should logically follow from the assessment.
If we’re worried about complication X (e.g. anastomotic leak), what are we doing to rule it out
- e.g. Assessment: ?anastomotic leak; Plan: NPO, r/a q4h, repeat labs, CT abdo/pelvis with oral/rectal contrast
- e.g. d/c home once pain controlled rather than writing CCM
5.4 OR Note
The PPP SAFE DISC mnemonic is widely used.
Preoperative diagnosis: as much as was known preoperatively
Postoperative diagnosis: usually ‘same’ in reference to preoperative diagnosis
Procedure
Surgeon
Assistants
Anesthetist (Name, type of anesthetic/airway)
Findings: anything notable about the case that someone might want to know about for future operative, inpatient, or outpatient care
Estimated blood loss (EBL)
Drains: internal/external location of drains, a diagram can help
Ins: for big cases, quantity of blood product/fluids administered
Specimens
Complications
Plan: postop destination, plan re:feeding, antibiotics, anticoagulants, discharge
The PPP SAFE DISC mnemonic is widely used.
Preoperative diagnosis: as much as was known preoperatively
Postoperative diagnosis: usually ‘same’ in reference to preoperative diagnosis
Procedure
Surgeon
Assistants
Anesthetist (Name, type of anesthetic/airway)
Findings: anything notable about the case that someone might want to know about for future operative, inpatient, or outpatient care
Estimated blood loss (EBL)
Drains: internal/external location of drains, a diagram can help
Ins: for big cases, quantity of blood product/fluids administered
Specimens
Complications
Plan: postop destination, plan re:feeding, antibiotics, anticoagulants, discharge